Joe is a 15-year-old who has been feeling “off” for several months. A tough quiz or an awkward social moment turns into something that he obsessively replays. He has trouble falling asleep and often wakes up at 3 a.m. worrying about the upcoming day. His score on the GAD-7, a clinical measure of anxiety, is 12; his pediatrician tells his mom that qualifies as “moderately anxious.”
Mom decides to act. The pediatrician gives her a referral for therapy and tells her to check Psychology Today’s online directory of providers. Mom finds several nearby professionals. One describes herself as a specialist in cognitive behavioral therapy, or CBT. Another claims to be an expert in an “eclectic” therapy. Still another uses something called dialectical behavioral therapy. She is choosing, she believes, among methods. The CBT description sounds the most sensible to her, so she goes with that. The waiting time is eight weeks.
What she doesn’t yet realize is that the person she gets for Joe will matter far more than the method. Behind one door is a CBT therapist who will leave Joe slightly worse, drifting up from 12 to 13 on the GAD-7. Behind another is a CBT therapist who will bring meaningful relief, moving him down to 8. And behind a third is an amazing CBT therapist who will produce something like remission, reducing Joe to a score of 4.
Which is which? Joe’s mom cannot tell from Psychology Today.
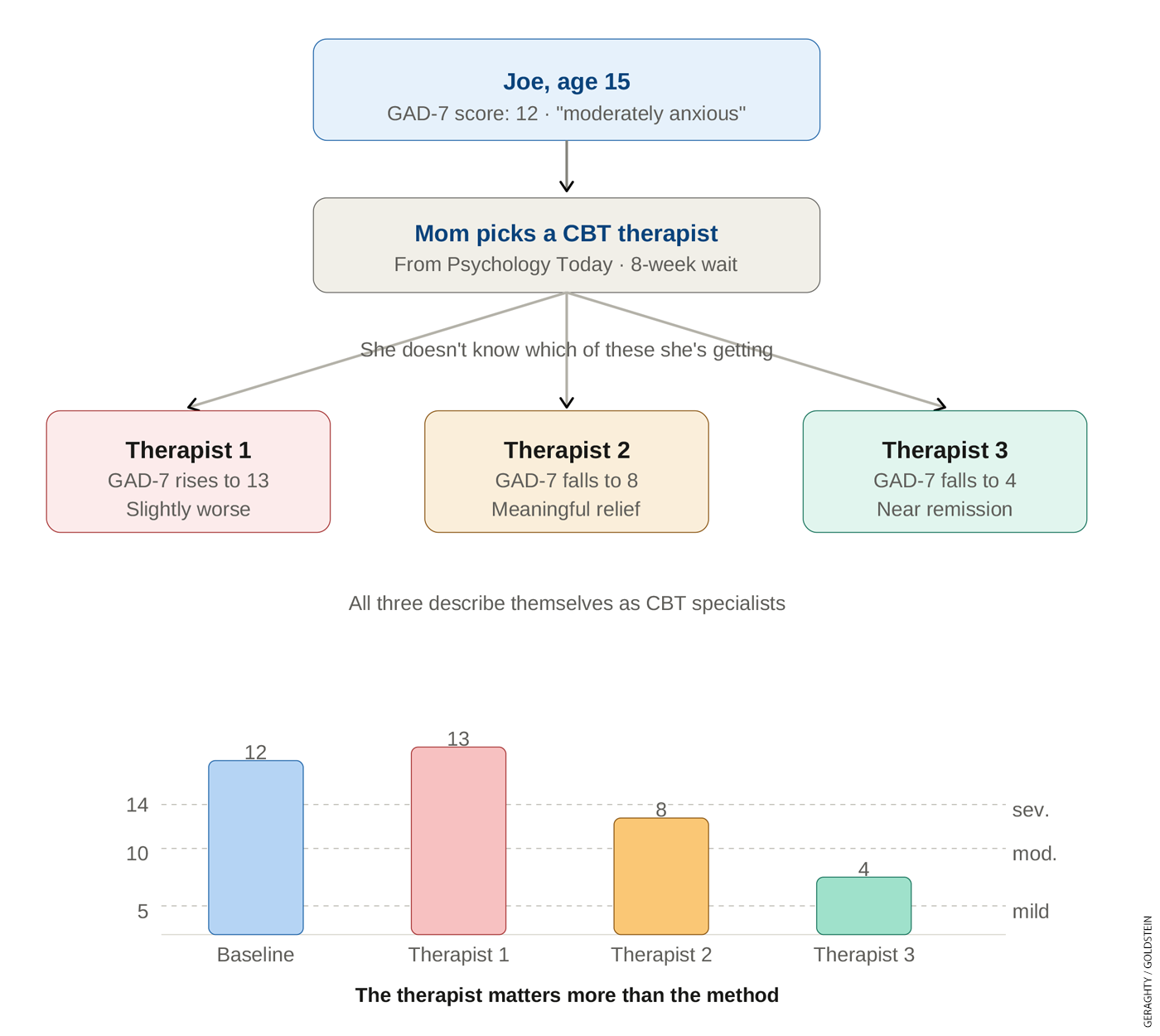
Research shows that different types of treatment for teen mental health concerns often produce roughly equivalent outcomes. The difference between Joe scoring 13 or 4 is much more likely to reflect the therapist than the method.
In short: Some therapists are much more effective than others. Treatment type accounts for at most one percent of the variance in patient outcomes. Therapist identity accounts for five to eight percent. The gap between a 90th-percentile therapist and a 50th-percentile therapist is meaningful, but the mental health care system doesn’t particularly want to know or act upon that information.
“There is no other profession where your performance is so ignored.”
Bruce Wampold is emeritus professor of counseling psychology at the University of Wisconsin and director of the Research Institute at Modum Bad Psychiatric Center in Norway. He has spent much of his career establishing, repeatedly, that who the therapist is matters more than what kind of therapy they use.
Wampold is direct. “There is no other profession where your performance is so ignored as psychotherapy,” he noted in a recent interview. On the research literature itself: “There have been 10,000 to 15,000 clinical trials of different psychotherapies. There have been maybe 20 studies of therapists. Amazing, isn’t it, when you think about the money spent?” Indeed, when Wampold sought funding from the National Institute of Mental Health to study individual therapists, he was denied.
The medical system relies on therapists’ credentials as proxies for quality. Are they predictive of results? No. Advanced degrees and additional certifications are weak predictors of patient outcomes—a result that will not surprise Education Next readers who have lived through analogous discussions about teachers.
What about experience? A longitudinal study following 170 therapists over up to 18 years found that therapist effectiveness drifted slightly downward as experience accumulated.
But maybe the scholars are mismeasuring therapists? After all, some deal with much tougher cases than others. An important study by David Saxon and Michael Barkham used statistical methods to control for case severity and patient risk. They wanted to test whether apparent therapist quality was just a reflection of caseload difficulty. The therapist effects persisted. Good ones still looked good. Struggling ones still looked bad. This is the same issue that methods to estimate “value-added” revealed for teachers.
A Familiar Reckoning: Therapist Quality and Teacher Quality
The Widget Effect, a 2009 report by The New Teacher Project, argued that schools were treating teachers as interchangeable parts, as though one were the same as any other. Everyone was rated satisfactory.
The report hit at a moment of political opportunity. President Obama’s Race to the Top grant program made improving teacher quality a top priority. The Gates Foundation had launched the Measures of Effective Teaching project, which aimed to develop a fair and reliable way of distinguishing teacher quality. The technocratic stuff went reasonably well, as Thomas Kane reported: “We showed that if you combine data from three different sources, you can identify teachers who cause greater learning to happen.”
But the politics?
Not so good, as Chad Aldeman’s careful postmortem here in Education Next demonstrates. Aldeman points to research by Matthew Kraft, who compiled ratings across the 24 states that had built new evaluation systems and found that in the vast majority of them, fewer than one percent of teachers landed in the lowest category.
The systems had nominally changed, but to little practical impact. Why? “No amount of investment in new evaluation systems would ever make teachers comfortable with consequential decisions flowing from those systems,” Aldeman wrote.
Today’s therapists are in a similar position. From their point of view, there are already several built-in forms of accountability. Patients can choose not to show up in the first place or not to return. A practice manager can fire them. In cases of serious misconduct, a licensing board can dismiss them.
How would they react to a new idea: measuring them based on outcomes, controlling for all the proper externalities, celebrating and rewarding the best, and at least notifying and offering help to those with consistently bad outcomes, followed by the possibility of counseling them out after months or years with no improvement in outcomes? They would not react well. They entered a profession with one understanding of accountability already in place. Politically, it is implausible to change that understanding retroactively. Let’s not try.
An Opening
Here is where the teacher and therapist evaluation stories depart, and where there might be an opportunity to address the teen mental health challenge.
Put simply, we need a lot more mental health providers. Schools have teacher shortages in some places, but nothing comparable to this. Six in ten psychologists aren’t taking new patients. The average wait for care is 48 days, and longer if you’re in a rural area, where a family often can’t find anyone who treats teenagers at all. While there are over a million behavioral health providers in the U.S., they are unevenly distributed. More than half of Americans (169 million) live somewhere the federal government has formally designated a “Mental Health Professional Shortage Area.”
There’s a policy opportunity here, and a few states have started to take it. California has created Certified Wellness Coaches, a new provider role with lighter credentialing, and Georgia has built a youth peer specialist model staffed by young adults with lived experience. Most state activity, though, has gone toward hiring more of the existing licensed workforce rather than testing new kinds of help.
EdNext in your inbox
Sign up for the EdNext Weekly newsletter, and stay up to date with the Daily Digest, delivered straight to your inbox.
We think this is a mistake. Three categories of alternative providers show promise, each resting on an encouraging evidence base. They could “enter fresh,” with little incumbent expectation of being treated like interchangeable widgets and no settled bargain to protect. That is the opening. With alternative providers, we could focus on patient outcomes, not inputs. We could trade low barriers to entry in exchange for accountability for patient improvement. Leave the traditional clinicians alone but measure the newcomers on their results.
Paraprofessionals. The evidence that formal clinical training produces better therapy is surprisingly thin, and it has been contested since Joseph Durlak first raised the question in 1979. In the most recent and most careful synthesis, a 2024 review by Smith, Hall, and Verona found that licensed professionals do not hold an edge in the treatment of children and adolescents. Paraprofessionals do their best work when they are trained in a structured intervention; behavioral activation, for example, produced strong results when delivered by unlicensed providers.
Chatbots. A 2026 meta-analysis pooled 39 randomized trials of chatbots and found moderate reductions in depression and anxiety. Therabot, a generative AI chatbot out of Dartmouth, was found to reduce users’ depressive symptoms by 51 percent in a New England Journal of Medicine study. Patients also rated their bond with the bot about the same as they would with a human. Of course, using these with teenagers would require a careful rollout; hundreds of bills to limit minors’ interactions with chatbots are pending in state legislatures in 2026.
Peer and Near-Peer Support. This approach rests on a simple intuition and has a growing evidence base. A 17-year-old may more readily connect with a “near-peer,” someone close enough to her own life to recognize what she’s going through, than with a 54 year-old licensed clinician. A 2025 JAMA Psychiatry viewpoint makes the case for integrating peers into care to ease the workforce shortage, and a 2025 review found some encouraging effects, particularly for eating disorders.
* * *
What if we invested in all these new provider types at once—and made outcome tracking a condition of the funding from the very start? We’d build the evidence we’re missing and likely get help to teens who can’t find any right now. Earlier we argued why outcome measurement collapsed for teachers, who objected to terms imposed on them years into the job. These providers would be different, because measurement is simply part of the bargain they sign up for on day one.
We could study this new cohort of providers and learn. Therapy, in turn, gets its Doug Lemov moment, a rigorous blueprint for what excellent providers do that others don’t. The National Institute of Mental Health could fund the evaluation infrastructure for which Wampold has advocated for over 30 years.
Joe and his mom? They’re no longer browsing Psychology Today and crossing their fingers. They now have much more varied choice. Maybe they still opt for the licensed CBT provider, or perhaps they try the new local practice that just opened, the one with young paraprofessionals trained in behavioral activation. Or maybe Joe uses a large language model to ease into seeing a provider as he waits for the right fit.
Open the door to new kinds of providers and measure their results from the start. In doing so, we can work on supply and quality at the same time.
Sean Geraghty and Mike Goldstein are the co-founders of the Center For Teen Flourishing.